 In 2004, the effects of our son’s disabilities spiralled into serious illness and constant pain. As a caregiver and mother, I was raw and vulnerable – it was the worst of times. I remember saying to doctors and family members, “I need you to be kind to me. I really need that.”
In 2004, the effects of our son’s disabilities spiralled into serious illness and constant pain. As a caregiver and mother, I was raw and vulnerable – it was the worst of times. I remember saying to doctors and family members, “I need you to be kind to me. I really need that.”
The problem with kindness is that it is no longer a public virtue. We assume that it will be there when we suffer and need it the most, but will it?
Today, kindness is endangered by the race towards independence and self-reliance, those old enemies of illness, babies, disability and aging. It has become synonymous with weakness in a culture that values the self over others. Reading about what constitutes winning in business, it’s easy to conclude that kindness is for losers.
Against that cultural background, it’s no wonder that natural care is not valued in our society. Caregivers are daily practitioners of kindness. We know how to comfort without calling attention to frailty. We’ve memorized recipes for favourite soups and casseroles. We reminisce, even when the dishes need clearing up or work deadlines loom. All these acts of caring kindness take time and their reward isn’t money – it’s love and satisfaction.
Teach kindness and relationships will grow by Gerry Chidiac
But we caregivers need kindness shown to us, too, to nurture and sustain us in our caring roles.
Kindness isn’t only about comfort and joy. Science has shown that it has real, healing benefits. Caregivers know this both from intuition and experience.
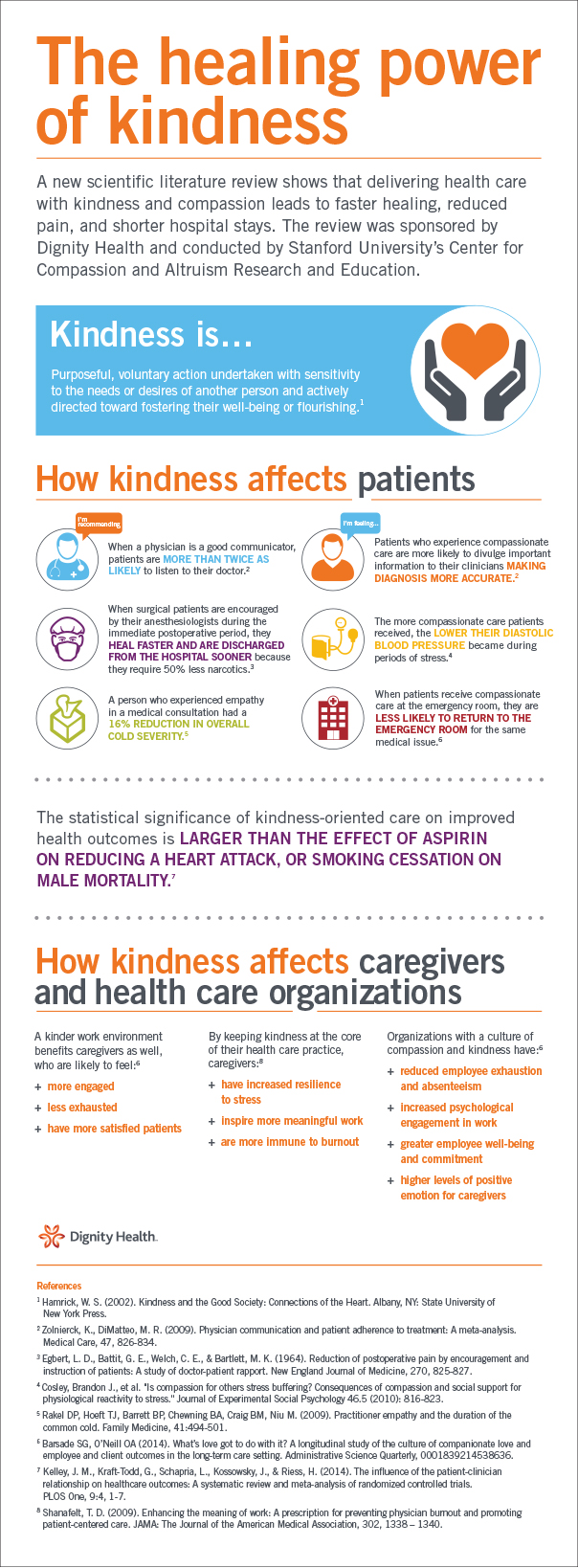
The Centre for Compassionate and Altruism Research and Education at Stanford University has revealed a growing body of evidence showing that kindness exhibited by healthcare professionals can lead to patients experiencing faster healing of wounds and reduced pain, anxiety and blood pressure, leading to shorter hospital stays.
A 2011 study showed that when physicians sat by patients’ bedsides, those patients reported a greater sense of being cared for than when physicians stood. Simply sitting was interpreted as compassionate listening. Patients whose doctors sat beside them recalled the physicians staying longer, even though in the study, doctors standing spent equal time by the bedside.
When the neurologist sat beside me to explain that our son had epilepsy, she saw my tears. I remember she pressed a tissue into my hand and when I looked up, our eyes met. “You will all be all right,” she said. I believed her.
And yet in medicine, kindness has evolved into the soft enemy of science. Good clinical care often has no place for long conversations or tears and hugs. Health-care professionals may be wary of kindness, as though there are risks attached to it – as though it is a kind of temptation – which indeed it is, because kindness gives us pleasure. Yet it’s our guilty pleasure, largely because we fear that it might sabotage our self-image of toughness, the core ingredient of success.
But once we decide to be kind, we become porous enough to be less isolated. We find ourselves experiencing belonging. This magical transaction is what caregivers, paid or unpaid, have to teach the rest of society. It’s as if the act of caring with love, in the presence of suffering, is a rite of passage and an important developmental achievement. In short, only an adult who has learned to bear frustration is capable of putting the needs of someone else before their own.
We all need kindness badly and we must discover the language to support it at home, work, hospital or wider community. Kindness needs to be taught, modelled, supported and championed as a primary virtue. Hospitals should have kindness standards and compliance requirements as they do for proper hand washing.
No one is immune from the positive effects of compassion and those who have allowed vulnerability to inform their confidence know that personal strength is their prize. Caregivers in our society are the wise elders who enact the virtues of maturity, character, compassion and kindness every day.
We are the purveyors of kindness but we need it shown to us, too.
Donna Thomson is a caregiver, author and activist. She wrote The Four Walls of My Freedom: Lessons I’ve Learned From a Life of Caregiving (2014) and blogs at The Caregivers’ Living Room (www.donnathomson.com). She is a board director of the Kids Brain Health Network and advises from a family perspective on numerous health research projects. She also teaches families how to advocate for care at The Advocacy School and The Caregiver Network. She writes Caring Connections with Vickie Cammack.
Donna is a Troy Media contributor. Why aren’t you?
![]()
The views, opinions and positions expressed by columnists and contributors are the author’s alone. They do not inherently or expressly reflect the views, opinions and/or positions of our publication.
A message from our Editor
An aging Canadian population and smaller families, combined with reduced health and social care budgets, mean the challenges of providing care to seniors will only worsen. Legions of families are buckling under the emotional, physical and fiscal burdens of caregiving. These pressures will be exacerbated by growing numbers of people living with demanding health challenges such as dementia, with fewer and fewer people to take care of them. The natural web of caring that so many of us take for granted is at risk of unravelling. Troy Media’s Family Ties examines the issues facing caregivers and the healthcare system in general and seeks solutions. If you have a story to tell, contact us at [email protected].






{kind=link}
0 Comments